Abstract
Background: Many severe asthma patients with high oral corticosteroid exposure (HOCS) often do not initiate biologics despite being eligible. This study aimed to compare the characteristics of severe asthma patients with HOCS who did and did not initiate biologics.
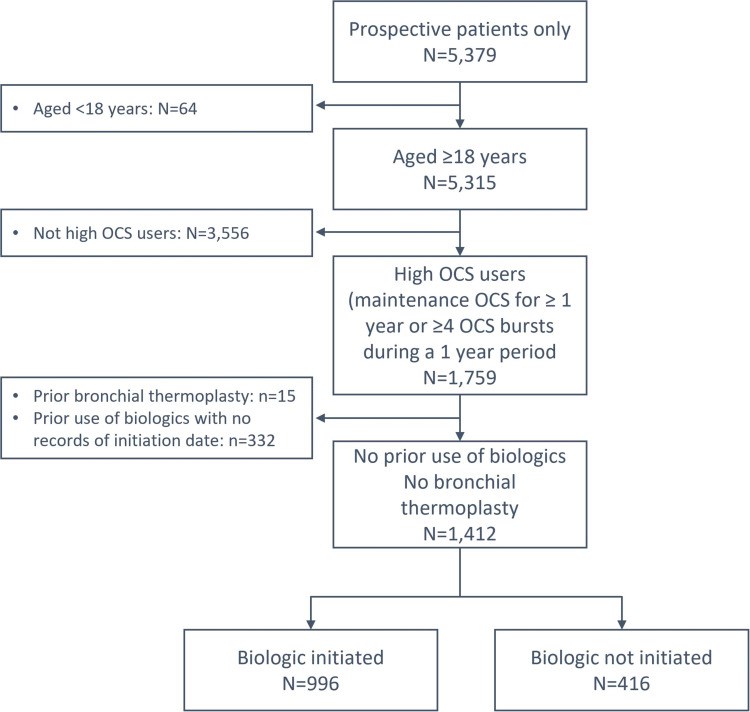
Methods: Baseline characteristics of patients with HOCS (long-term maintenance OCS therapy for at least 1 year, or ≥4 courses of steroid bursts in a year) from the International Severe Asthma Registry (ISAR; https://isaregistries.org/), who initiated or did not initiate biologics (anti-lgE, anti-IL5/5R or anti-IL4R), were described at the time of biologic initiation or registry enrolment. Statistical relationships were tested using Pearson's chi-squared tests for categorical variables, and t-tests for continuous variables, adjusting for potential errors in multiple comparisons.
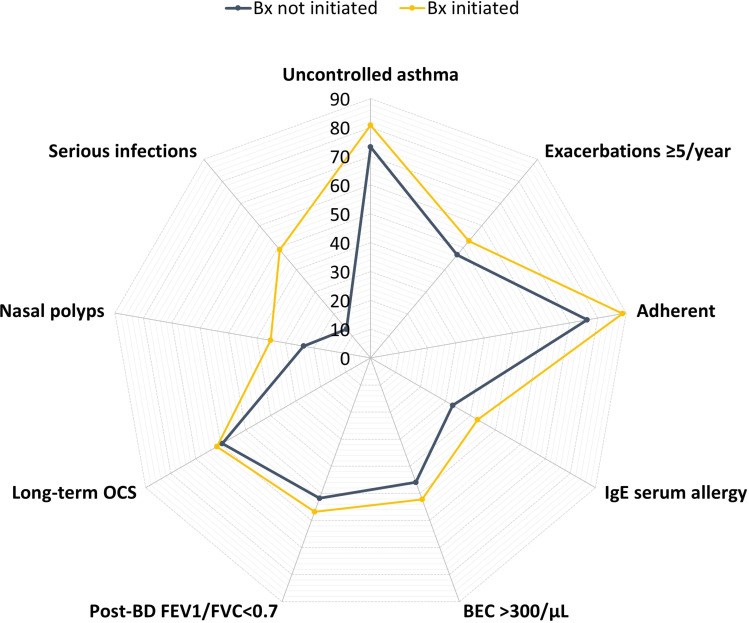
Results: Between January 2015 and February 2021, we identified 1412 adult patients with severe asthma from 19 countries that met our inclusion criteria of HOCS, of whom 996 (70.5%) initiated a biologic and 416 (29.5%) did not. The frequency of biologic initiation varied across geographical regions. Those who initiated a biologic were more likely to have higher blood eosinophil count (483 vs 399 cells/µL, p=0.003), serious infections (49.0% vs 13.3%, p<0.001), nasal polyps (35.2% vs 23.6%, p<0.001), airflow limitation (56.8% vs 51.8%, p=0.013), and uncontrolled asthma (80.8% vs 73.2%, p=0.004) despite greater conventional treatment adherence than those who did not start a biologic. Both groups had similar annual asthma exacerbation rates in the previous 12 months (5.7 vs 5.3, p=0.147).
Conclusion: Around one third of severe HOCS asthma patients did not receive biologics despite a similar high burden of asthma exacerbations as those who initiated a biologic therapy. Other disease characteristics such as eosinophilic phenotype, serious infectious events, nasal polyps, airflow limitation and lack of asthma control appear to dictate biologic use.
Keywords: biologics; patient characteristics; real-world; severe asthma; treatment pattern.
Conflict of interest statement
Mohsen Sadatsafavi has received honoraria from AZ, BI, and GSK for purposes unrelated to the content of this manuscript and has received research funding from AZ and BI directly into his research account from AZ for unrelated projects. Trung N. Tran is an employee of AstraZeneca. AstraZeneca is a co-funder of the International Severe Asthma Registry. Nigel Chong Boon Wong reports grants from Optimum Patient Care Global, grants from AstraZeneca Ltd, during the conduct of the study. Nasloon Ali was an employee of Observational and Pragmatic Research Institute (OPRI) at the time this research was conducted. OPRI conducted this study in collaboration with Optimum Patient Care and AstraZeneca. Con Ariti is an employee of the Observational and Pragmatic Research Institute (OPRI). OPRI conducted this study in collaboration with Optimum Patient Care and AstraZeneca. Esther Garcia Gil was an employee of AstraZeneca at the time this research was conducted. AstraZeneca is a co-funder of the International Severe Asthma Registry. Anthony Newell was an employee of Optimum Patient Care (OPC) at the time this research was conducted. OPC is a co-funder of the International Severe Asthma Registry. Marianna Alacqua was an employee of AstraZeneca at the time this research was conducted. AstraZeneca is a co-funder of the International Severe Asthma Registry. Mona Al-Ahmad has received advisory board and speaker fees from AstraZeneca, Sanofi, Novartis, and GlaxoSmithKline. Alan Altraja has received lecture fees from AstraZeneca, Berlin-Chemie Menarini, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, MSD, Norameda, Novartis, Orion, Sanofi, and Zentiva; personal fees from Teva, Shire Pharmaceuticals and CSL Behring, sponsorships from AstraZeneca, Berlin-Chemie Menarini, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, MSD, Norameda, Sanofi, and Novartis; and has been a member of advisory boards for AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Novartis, Sanofi, and Teva. Riyad Al-Lehebi has given lectures at meetings supported by AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, and Sanofi, reports personal fees from Novartis and participated in advisory board fees from GlaxoSmithKline. Mohit Bhutani: has received advisory board and speaker fees from AstraZeneca, GlaxoSmithKline, Pfizer, Sanofi Genzyme, Covis pharmaceuticals; has been an investigator on clinical trials sponsored by AstraZeneca, GlaxoSmithKline, Sanofi Genzyme, Boehringer Ingelheim Leif Bjermer has (in the last three years) received lecture or advisory board fees from Alk-Abello, AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Mundipharma, Novartis, Sanofi, Genzyme/Regeneron, and Teva. Anne-Sofie Bjerrum has received lecture fees from Astra Zeneca, GlaxoSmithKline, Novartis. Arnaud Bourdin has received industry-sponsored grants from AstraZeneca-MedImmune, Boehringer-Ingelheim, Cephalon/Teva, GlaxoSmithKline, Novartis, Sanofi-Regeneron and consultancies with AstraZeneca-MedImmune, Boehringer-Ingelheim, GlaxoSmithKline, Novartis, Regeneron-Sanofi, Med-in-Cell, Actelion, Merck, Roche, and Chiesi. Lakmini Bulathsinhala is an employee of the Observational and Pragmatic Research Institute (OPRI). OPRI conducted this study in collaboration with Optimum Patient Care and AstraZeneca. Anna von Bülow reports speakers fees and consultancy fees from AstraZeneca, GSK and Novartis, outside the submitted work. She has also attended advisory board for Novartis and AstraZeneca. John Busby reports personal fees from NuvoAir, outside the submitted work. Giorgio Walter Canonica has received research grants, as well as lecture or advisory board fees from A. Menarini, Alk-Albello, Allergy Therapeutics, Anallergo, AstraZeneca, MedImmune, Boehringer Ingelheim, Chiesi Farmaceutici, Circassia, Danone, Faes, Genentech, Guidotti Malesci, GlaxoSmithKline, Hal Allergy, Merck, MSD, Mundipharma, Novartis, Orion, Sanofi Aventis, Sanofi, Genzyme/Regeneron, Stallergenes, UCB Pharma, Uriach Pharma, Teva, Thermo Fisher, and Valeas. Victoria Carter is an employee of Optimum Patient Care, a co-funder of the International Severe Asthma Registry and reports grants from Optimum Patient Care Global, during the conduct of the study Borja G. Cosio declares grants from Chiesi, AstraZeneca, Menarini, Teva and GSK; personal fees for advisory board activities from Chiesi, GSK, Novartis, Sanofi, Menarini, Teva and AstraZeneca; and payment for lectures/speaking engagements from Chiesi, Novartis, GSK, Menarini, Sanofi, Teva and AstraZeneca, outside the submitted work. Richard W. Costello has received honoraria for lectures from Aerogen, AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Novartis, and Teva. He is a member of advisory boards for GlaxoSmithKline and Novartis, has received grant support from GlaxoSmithKline and Aerogen, has received personal fees from Respirasense, personal fees from PfizerBioNTech, during the conduct of the study and has patents in the use of acoustics in the diagnosis of lung disease, assessment of adherence and prediction of exacerbations, issued to 212. J. Mark FitzGerald reports grants from AstraZeneca, GSK, Sanofi Regeneron, Novartis paid directly to UBC. Personal fees for lectures and attending advisory boards: AstraZeneca, GSK, Sanofi Regeneron, TEVA. João A Fonseca reports grants from or research agreements with AstraZeneca, Mundipharma, Sanofi Regeneron and Novartis. Personal fees for lectures and attending advisory boards: AstraZeneca, GSK, Mundipharma, Novartis, Sanofi Regeneron and TEVA. Liam G. Heaney declares he has received grant funding, participated in advisory boards and given lectures at meetings supported by Amgen, AstraZeneca, Boehringer Ingelheim, Circassia, Evelo Biosciences, Hoffmann la Roche, GlaxoSmithKline, Novartis, Theravance and Teva; he has taken part in asthma clinical trials sponsored by Boehringer Ingelheim, Hoffmann la Roche, and GlaxoSmithKline for which his institution received remuneration; he is the Academic Lead for the Medical Research Council Stratified Medicine UK Consortium in Severe Asthma which involves industrial partnerships with a number of pharmaceutical companies including Amgen, AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Hoffmann la Roche, and Janssen. Enrico Heffler participates in speaking activities and industry advisory committees for AstraZeneca, Sanofi-Genzyme, GSK, Novartis, Regeneron, Stallergenes-Greer, TEVA, Circassia and Nestlè Purina, grants from AstraZeneca and GSK Mark Hew declares grants and other advisory board fees (made to his institutional employer) from AstraZeneca, GlaxoSmithKline, Novartis, Sanofi, and Seqirus, for unrelated projects. Flavia Hoyte declares honoraria from AstraZeneca. She has been an investigator on clinical trials sponsored by GlaxoSmithKline, Genentech, Teva, Sanofi and National Institute of Allergy and Infectious Diseases (NIAID), for which her institution has received funding. Takashi Iwanaga declares grants from Astellas, Boehringer Ingelheim, Daiichi-Sankyo, Kyorin, MeijiSeika Pharma, Teijin Pharma, Ono, and Taiho, and lecture fees from Kyorin, GlaxoSmithKline, Sanofi and AstraZeneca. David J. Jackson has received advisory board and speaker fees from AstraZeneca, GlaxoSmithKline, Boehringer Ingelheim, Teva, Napp, Chiesi, Sanofi Regeneron, Novartis and research grant funding from AstraZeneca. Rupert C. Jones declares grants from Astra Zeneca, Glaxo Smith Kline, Novartis OPRI and Teva and personal fees for consultancy, speakers’ fees or travel support from Astra Zeneca, Boehringer Ingelheim, Glaxo Smith Kline, Novartis and OPRI. Mariko Siyue Koh reports grant support from AstraZeneca, and honoraria for lectures and advisory board meetings paid to her hospital (Singapore General Hospital) from GlaxoSmithKline, AstraZeneca, Sanofi and Boehringer Ingelheim, outside the submitted work. Piotr Kuna reports personal fees from Adamed, personal fees from AstraZeneca, personal fees from Berlin Chemie Manarini, personal fees from Boehringer Ingelheim, personal fees from Lekam, personal fees from Novartis, personal fees from Chiesi, personal fees from Polpharma, personal fees from Sanofi, personal fees from Teva, personal fees from Zentiva, personal fees from FAES, personal fees from Glenmark, outside the submitted work Désirée Larenas Linnemann reports speaker or personal fees from ALK, Alakos, Armstrong, AstraZeneca, Boehringer Ingelheim, Chiesi, DBV Technologies, Gossamer, Grunenthal, GSK, Mylan/Viatris, Menarini, MSD, Novartis, Pfizer, Purina institute, Sanofi, Siegfried, UCB, Carnot, Viatris, and grants from Sanofi, AbbVie, ALK, AstraZeneca, Circassia, Chiesi, GSK, Lilly, Novartis, Pfizer, Purina Institute and UCB, outside the submitted work Sverre Lehmann declares receipt of lecture (personal) and advisory board (to employer) fees from AstraZeneca, Boehringer Ingelheim, and Novartis. Lauri A. Lehtimäki declares personal fees for consultancy, lectures and attending advisory boards from ALK, AstraZeneca, Boehringer Ingelheim, Circassia, Chiesi, GlaxoSmithKline, Mundipharma, Novartis, Orion Pharma, Sanofi, and Teva. Juntao Lyu is an employee of Optimum Patient Care (OPC). OPC is a co-funder of the International Severe Asthma Registry. Jorge Maspero reports grants and personal fees from AstraZeneca, Sanofi, Novartis, and GSK, personal fees from IMMUNOTEK, personal fees from SANOFI, outside the submitted work. Andrew N. Menzies-Gow has attended advisory boards for AstraZeneca, GlaxoSmithKline, Novartis, Regeneron, Sanofi and Teva, andhas received speaker fees from AstraZeneca, Novartis, Teva and Sanofi. He has participated in research with AstraZeneca for which his institution has been remunerated and has attended international conferences with Teva. He has had consultancy agreements with AstraZeneca and Sanofi. Nikolaos G. Papadopoulos declares research support from Gerolymatos, Menarini, Nutricia, and Vian; and consultancy/speaker fees from ASIT, AZ, Boehringer Ingelheim, GSK, HAL Allergy, Medscape, Menarini, MSD, Mylan, Novartis, and Nutricia, OM Pharma, Sanofi, and Takeda, grant from Capricare. Andriana I. Papaioannou has received fees and honoraria from Menarini, GSK, Novartis, Elpen, Boehringer Ingelheim, AstraZeneca, and Chiesi. Luis Perez-de-Llano declares non-financial support, personal fees, and grants from Teva, Sanofi and AstraZeneca, Chesi; non-financial support and personal fees from Boehringer Ingelheim, Esteve, GlaxoSmithKline, Mundipharma, and Novartis; personal fees from MSD, TECHDOW PHARMA, Leo-Pharma, GEBRO and GILEAD; non-financial support from Menairi, grants, non-financial support from FAES during the conduct of the study. Diahn-Warng Perng (Steve) received sponsorship to attend or speak at international meetings, honoraria for lecturing or attending advisory boards, and research grants from the following companies: AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Novartis, Daiichi Sankyo, Shionogi and Orient Pharma Matthew Peters declares personal fees and non-financial support from AstraZeneca and GlaxoSmithKline. Paul E. Pfeffer has attended advisory boards for AstraZeneca, Sanofi and GSK; has given lectures at meetings supported by AstraZeneca and GlaxoSmithKline; has taken part in clinical trials sponsored by AstraZeneca, GlaxoSmithKline, Sanofi and Novartis, for which his institution received remuneration; non-financial support from Chiesi; and has a current research grant funded by GlaxoSmithKline. Celeste M. Porsbjerg has attended advisory boards for AstraZeneca, Novartis, TEVA, and Sanofi-Genzyme; has given lectures at meetings supported by AstraZeneca, Novartis, TEVA, Sanofi-Genzyme, and GlaxoSmithKline; has taken part in clinical trials sponsored by AstraZeneca, Novartis, MSD, Sanofi-Genzyme, GlaxoSmithKline, and Novartis; and has received educational and research grants from AstraZeneca, Novartis, TEVA, GlaxoSmithKline, ALK, and Sanofi-Genzyme. Todor A. Popov declares relevant research support from Novartis and Chiesi Pharma. Chin Kook Rhee declares consultancy and lecture fees from AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Mundipharma, MSD, Novartis, Sandoz, Sanofi, Takeda, and Teva-Handok. Sundeep Salvi declares research support and speaker fees from Cipla, Glenmark, GSK Camille Taillé has received lecture or advisory board fees and grants to her institution from AstraZeneca, Sanofi, GlaxoSmithKline, Chiesi and Novartis, for unrelated projects. Carlos A. Torres-Duque has received fees as advisory board participant and/or speaker from AstraZeneca, Boehringer-Ingelheim, GlaxoSmithKline, Novartis, and Sanofi-Aventis; has taken part in clinical trials from AstraZeneca, Novartis and Sanofi-Aventis; has received unrestricted grants for investigator-initiated studies at Fundacion Neumologica Colombiana from AstraZeneca, Boehringer-Ingelheim, GlaxoSmithKline, Grifols and Novartis. Charlotte S. Ulrik has attended advisory boards for AstraZeneca, ALK-Abello, GSK, Boehringer-Ingelheim, Novartis, Chiesi, TEVA, and Sanofi-Genzyme; has given lectures at meetings supported by AstraZeneca, Sandoz, Mundipharma, Chiesi, Boehringer-Ingelheim, Orion Pharma, Novartis, TEVA, Sanofi-Genzyme, and GlaxoSmithKline; has taken part in clinical trials sponsored by AstraZeneca, Novartis, Merck, InsMed, ALK-Abello, Sanofi-Genzyme, GlaxoSmithKline, Boehringer-Ingelheim, Regeneron, Chiesi and Novartis; and has received educational and research grants from AstraZeneca, MundiPharma, Boehringer-Ingelheim, Novartis, TEVA, GlaxoSmithKline and Sanofi-Genzyme; has received personal fees from Pfizer. Seung Won Ra has received lecture fees from AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, and Novartis. Eileen Wang has received honoraria from AstraZeneca, GlaxoSmithKline, Wefight, and Clinical Care Options. She has been an investigator on clinical trials sponsored by AstraZeneca, GlaxoSmithKline, Genentech, Novartis, Teva, and Sanofi, for which her institution has received funding. She has received personal fees from Wefight. Michael E. Wechsler reports receiving consulting honoraria from AstraZeneca, Boehringer Ingelheim, Genentech, GSK, Novartis, Regeneron, Sanofi and Teva; personal fees from Amgen, Avalo, Cerecor, Cytoreason, Eli Lilly, Equillium, Incyte, Kinaset, Phylaxis, Pulmatrix, Rapt and Sound Biologics. David B. Price has advisory board membership with Amgen, AstraZeneca, Boehringer Ingelheim, Chiesi, Circassia, Mylan, Mundipharma, Novartis, Regeneron Pharmaceuticals, Sanofi Genzyme, Teva Pharmaceuticals, Thermofisher; consultancy agreements with Amgen, AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Mylan, Mundipharma, Novartis, Pfizer, Teva Pharmaceuticals, Theravance; grants and unrestricted funding for investigator-initiated studies (conducted through Observational and Pragmatic Research Institute Pte Ltd) from AstraZeneca, Boehringer Ingelheim, Chiesi, Circassia, Mylan, Mundipharma, Novartis, Pfizer, Regeneron Pharmaceuticals, Respiratory Effectiveness Group, Sanofi Genzyme, Teva Pharmaceuticals, Theravance, UK National Health Service; payment for lectures/speaking engagements from AstraZeneca, Boehringer Ingelheim, Chiesi, Cipla, GlaxoSmithKline, Kyorin, Mylan, Mundipharma, Novartis, Regeneron Pharmaceuticals, Sanofi Genzyme, Teva Pharmaceuticals; payment for the development of educational materials from Mundipharma, Novartis; payment for travel/accommodation/meeting expenses from AstraZeneca, Boehringer Ingelheim, Mundipharma, Mylan, Novartis, Thermofisher; funding for patient enrolment or completion of research from Novartis; stock/stock options from AKL Research and Development Ltd which produces phytopharmaceuticals; owns 74% of the social enterprise Optimum Patient Care Ltd (Australia and UK) and 74% of Observational and Pragmatic Research Institute Pte Ltd (Singapore); 5% shareholding in Timestamp which develops adherence monitoring technology; is peer reviewer for grant committees of the Efficacy and Mechanism Evaluation programme, and Health Technology Assessment; and was an expert witness for GlaxoSmithKline. The authors report no other conflicts of interest in this work.