Oral Nystatin Prophylaxis for the Prevention of Fungal Colonization in Very Low Birth Weight Infants: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Figures
Similar articles
Austin N, Darlow BA, McGuire W.Cochrane Database Syst Rev. 2009 Oct 7;(4):CD003478. doi: 10.1002/14651858.CD003478.pub3.PMID: 19821309 Updated. Review.
Prophylactic oral antifungal agents to prevent systemic candida infection in preterm infants.
Austin NC, Darlow B.Cochrane Database Syst Rev. 2004;(1):CD003478. doi: 10.1002/14651858.CD003478.pub2.PMID: 14974017 Updated. Review.
Rundjan L, Wahyuningsih R, Oeswadi CA, Marsogi M, Purnamasari A.BMC Pediatr. 2020 Apr 17;20(1):170. doi: 10.1186/s12887-020-02074-0.PMID: 32303210 Free PMC article. Clinical Trial.
Austin N, Cleminson J, Darlow BA, McGuire W.Cochrane Database Syst Rev. 2015 Oct 24;2015(10):CD003478. doi: 10.1002/14651858.CD003478.pub5.PMID: 26497202 Free PMC article. Review.
Austin N, Darlow BA, McGuire W.Cochrane Database Syst Rev. 2013 Mar 28;(3):CD003478. doi: 10.1002/14651858.CD003478.pub4.PMID: 23543519 Updated. Review.
KMEL References
References
-
- Not just little adults: candidemia epidemiology, molecular characterization, and antifungal susceptibility in neonatal and pediatric patients. Blyth CC, Chen SC, Slavin MA, et al. Pediatrics. 2009;123:1360–1368. - PubMed
-
- Late-onset sepsis in very low birth weight neonates: the experience of the NICHD Neonatal Research Network. Stoll BJ, Hansen N, Fanaroff AA, et al. Pediatrics. 2002;110:285–291. - PubMed
-
- Epidemiological features of nosocomial candidaemia in neonates, infants and children: a multicentre study in Iran. Ahangarkani F, Shokohi T, Rezai MS, et al. Mycoses. 2020;63:382–394. - PubMed
-
- Nosocomial bloodstream infections in US hospitals: analysis of 24,179 cases from a prospective nationwide surveillance study. Wisplinghoff H, Bischoff T, Tallent SM, Seifert H, Wenzel RP, Edmond MB. Clin Infect Dis. 2004;39:309–317. - PubMed
-
- Neurodevelopmental and growth impairment among extremely low-birth-weight infants with neonatal infection. Stoll BJ, Hansen NI, Adams-Chapman I, Fanaroff AA, Hintz SR, Vohr B, Higgins RD. JAMA. 2004;292:2357–2365. - PubMed
-
- Oral nystatin prophylaxis to prevent invasive candidiasis in neonatal intensive care unit. Ozturk MA, Gunes T, Koklu E, Cetin N, Koc N. Mycoses. 2006;49:484–492. - PubMed
-
- London, England: Cochrane; 2022. Cochrane Handbook for Systematic Reviews of Interventions.
-
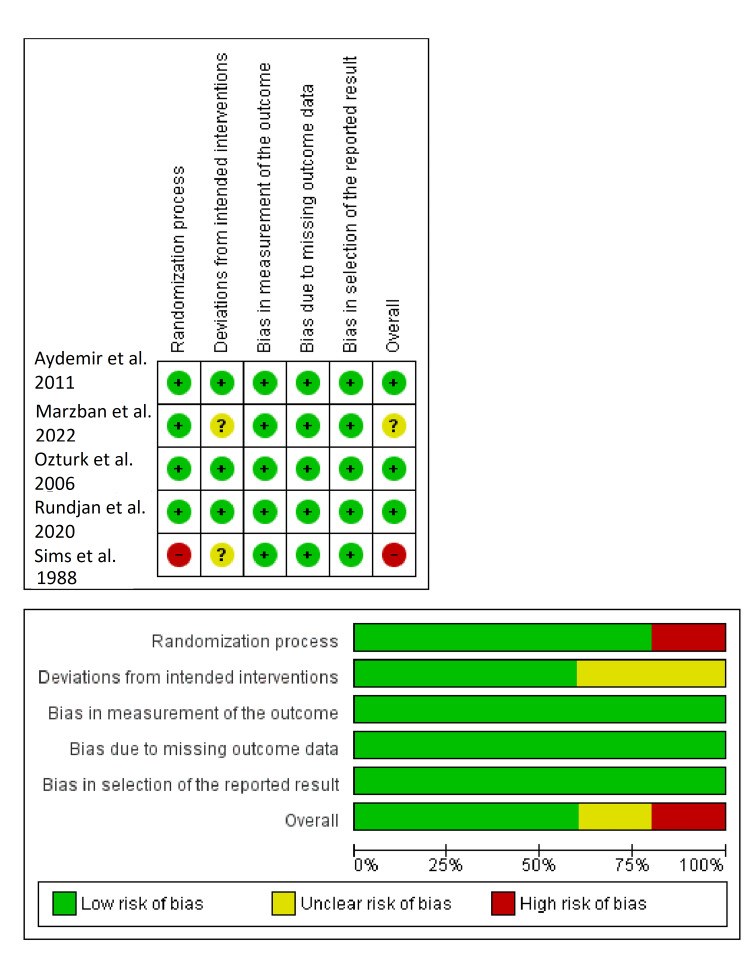
- RoB 2: a revised tool for assessing risk of bias in randomised trials. Sterne JA, Savović J, Page MJ, et al. BMJ. 2019;366 - PubMed
-
- Prophylactic oral nystatin and fungal infections in very-low-birthweight infants. Sims ME, Yoo Y, You H, Salminen C, Walther FJ. Am J Perinatol. 1988;5:33–36. - PubMed
-
- Randomised controlled trial of prophylactic fluconazole versus nystatin for the prevention of fungal colonisation and invasive fungal infection in very low birth weight infants. Aydemir C, Oguz SS, Dizdar EA, et al. Arch Dis Child Fetal Neonatal Ed. 2011;96:164–168. - PubMed
-
- Effectiveness of oral nystatin prophylaxis in the prevention of Candida colonization in very low birth weight preterm neonates; a randomized controlled trial. Marzban A, Aghdam MK, Ahadi S. https://ijn.mums.ac.ir/article_20231_8b10979d1f51d336501b4ec22608389c.pdf Iran J Neonatol. 2022;13:91–97.
-
- Clinical use of oral nystatin in the prevention of systemic candidosis in patients at particular risk. Schäfer-Korting M, Blechschmidt J, Korting HC. Mycoses. 1996;39:329–339. - PubMed
-
- Challenging issues in neonatal candidiasis. Kaufman DA. Curr Med Res Opin. 2010;26:1769–1778. - PubMed
-
- Prophylactic oral nystatin for preterm babies under 33 weeks' gestation decreases fungal colonisation and invasive fungaemia. Ganesan K, Harigopal S, Neal T, Yoxall CW. Arch Dis Child Fetal Neonatal Ed. 2009;94:275–278. - PubMed
-
- Oral nystatin prophylaxis and neonatal fungal infections. Howell A, Isaacs D, Halliday R. Arch Dis Child Fetal Neonatal Ed. 2009;94:429–433. - PubMed
-
- Chemoprophylaxis of neonatal fungal infections in very low birthweight infants: efficacy and safety of fluconazole and nystatin. Blyth CC, Barzi F, Hale K, Isaacs D. J Paediatr Child Health. 2012;48:846–851. - PubMed
-
- The global burden of fungal diseases. Vallabhaneni S, Mody RK, Walker T, Chiller T. Infect Dis Clin North Am. 2016;30:1–11. - PubMed