Division of Neurology, Department of Medicine, Amiri Hospital, Arabian Gulf Street, Sharq, 13041 Kuwait ; Neurology Clinic, Department of Medicine, Dasman Diabetes Institute, P.O. Box 1180, Dasman, 15462 Kuwait.
Department of Neurology, Ibn Sina Hospital, P.O. Box 25427, Safat, 13115 Kuwait ; Department of Neurology & Psychiatry, Al-Minia University Hospital, P.O. Box 61519, Minia, 61111 Egypt.
Department of Neurology, Ibn Sina Hospital, P.O. Box 25427, Safat, 13115 Kuwait.
Department of Neurology, Ibn Sina Hospital, P.O. Box 25427, Safat, 13115 Kuwait ; Department of Medicine, Kuwait University, P.O. Box 24923, Safat, 13110 Kuwait.
Background: Demyelinating plaques may induce headache through disruption of the pathways, which are implicated in the pathogeneses of migraine. We report a case of 25-year-old female patient, who presented with status migrainosus fulfilling the criteria of international classification of headache disorder. She was eventually diagnosed with multiple sclerosis (MS) after an extensive work-up and long-term clinical and radiological follow-up.
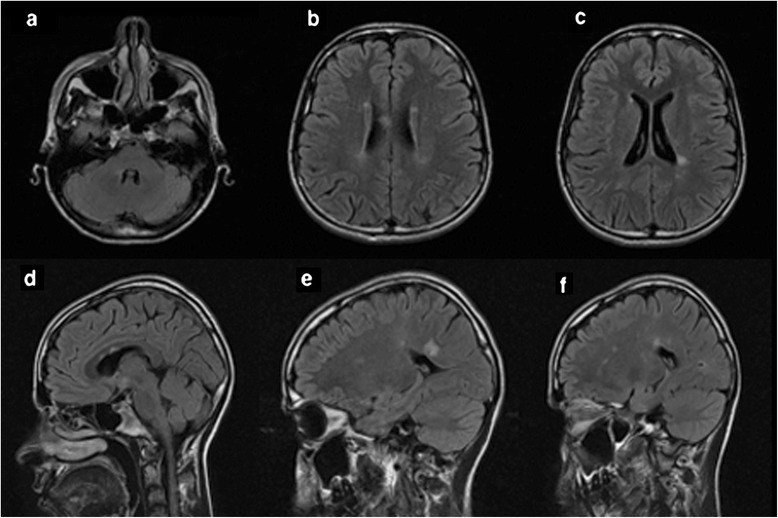
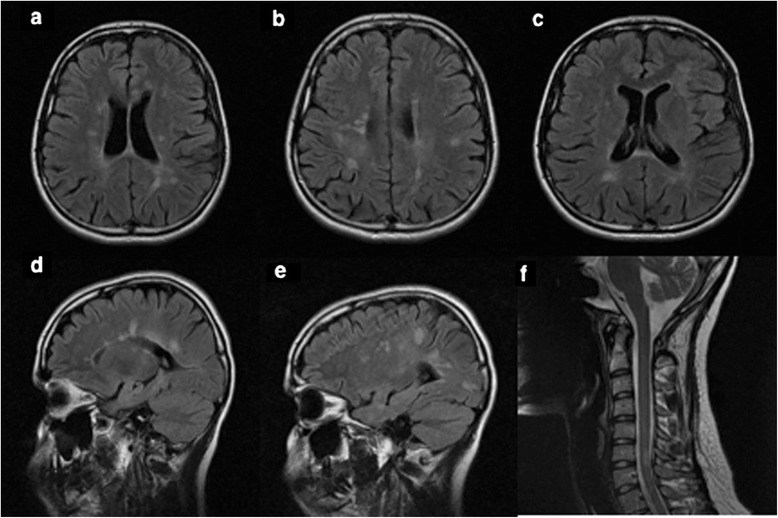
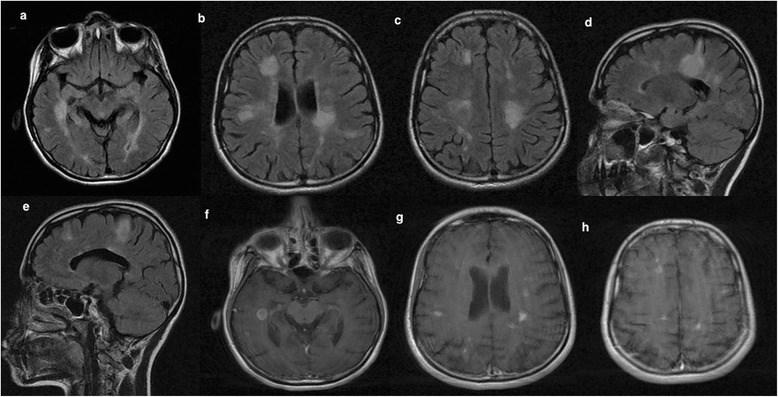
Findings: At the onset of status migrainosus, magnetic resonance imaging (MRI) revealed the presence of several demyelinating lesions fulfilling Swanton criteria. She was started on migraine prophylactic treatment but there was no subsequent response. One year later, she presented with recurrent status migrainosus and a follow-up MRI revealed multiple gadolinium-enhancing lesions in the brain. She was treated with abortive migraine medications. Within the following 2 year, she developed ascending parasthesia and weakness of both lower limbs indicative of incomplete transverse myelitis in association with recurrent status migrainosus. A diagnosis of MS was established based on a follow-up MRI that satisfied the revised 2010 McDonald criteria. Both the headache and neurological signs improved with IV methylprednisolone therapy. Her headache entered remission after initiation of a disease modifying therapy.
Conclusion: Status migrainosus can be the initial presentation of MS. Unresponsiveness to migraine prophylactic therapy in the presence of active demyelinating plaque in MRI brain may pose a diagnostic challenge and a diagnosis of MS might be considered.
Chen X, Zhang J, Li HL, Deng ZR, Wang L, Cao L, Xie CJ, Wang Y.Front Neurol. 2021 Mar 17;12:646029. doi: 10.3389/fneur.2021.646029. eCollection 2021.PMID: 33815258 Free PMC article.
Togha M, Abbasi Khoshsirat N, Moghadasi AN, Mousavinia F, Mozafari M, Neishaboury M, Mousavi SM.Iran J Neurol. 2016 Jan 5;15(1):1-8.PMID: 27141270 Free PMC article.
Fragoso YD, Brooks JB. Two cases of lesions in brainstem in multiple sclerosis and refractory migraine. Headache. 2007;47(6):852–854. doi: 10.1111/j.1526-4610.2007.00823.x. - DOI - PubMed
Freedman MS, Gray TA. Vascular headache: a presenting symptom of multiple sclerosis. Can J Neurol Sci. 1989;16(1):63–66. - PubMed
Gee JR, Chang J, Dublin AB, Vijayan N. The association of brainstem lesions with migraine-like headache: an imaging study of multiple sclerosis. Headache. 2005;45(6):670–677. doi: 10.1111/j.1526-4610.2005.05136.x. - DOI - PubMed
Goadsby PJ, Lipton RB, Ferrari MD. Migraine–current understanding and treatment. N Engl J Med. 2002;346(4):257–270. doi: 10.1056/NEJMra010917. - DOI - PubMed
Gursoy-Ozdemir Y, Qiu J, Matsuoka N, Bolay H, Bermpohl D, Jin H, Wang X, Rosenberg GA, Lo EH, Moskowitz MA. Cortical spreading depression activates and upregulates MMP-9. J Clin Invest. 2004;113(10):1447–1455. doi: 10.1172/JCI200421227. - DOI - PMC - PubMed
Headache Classification Committee of the International Headache S The International Classification of Headache Disorders, 3rd edition (beta version) Cephalalgia. 2013;33(9):629–808. doi: 10.1177/0333102413485658. - DOI - PubMed
Kister I, Caminero AB, Monteith TS, Soliman A, Bacon TE, Bacon JH, Kalina JT, Inglese M, Herbert J, Lipton RB. Migraine is comorbid with multiple sclerosis and associated with a more symptomatic MS course. J Headache Pain. 2010;11(5):417–425. doi: 10.1007/s10194-010-0237-9. - DOI - PMC - PubMed
Kister I, Caminero AB, Herbert J, Lipton RB. Tension-type headache and migraine in multiple sclerosis. Curr Pain Headache Rep. 2010;14(6):441–448. doi: 10.1007/s11916-010-0143-5. - DOI - PubMed
Kister I, Munger KL, Herbert J, Ascherio A. Increased risk of multiple sclerosis among women with migraine in the Nurses' Health Study II. Mult Scler. 2012;18(1):90–97. doi: 10.1177/1352458511416487. - DOI - PMC - PubMed
Lin GY, Wang CW, Chiang TT, Peng GS, Yang FC. Multiple sclerosis presenting initially with a worsening of migraine symptoms. J Headache Pain. 2013;14:70. doi: 10.1186/1129-2377-14-70. - DOI - PMC - PubMed
Merkler D, Klinker F, Jurgens T, Glaser R, Paulus W, Brinkmann BG, Sereda MW, Stadelmann-Nessler C, Guedes RC, Bruck W, Liebetanz D. Propagation of spreading depression inversely correlates with cortical myelin content. Ann Neurol. 2009;66(3):355–365. doi: 10.1002/ana.21746. - DOI - PubMed
Noseworthy JH, Lucchinetti C, Rodriguez M, Weinshenker BG. Multiple sclerosis. N Engl J Med. 2000;343(13):938–952. doi: 10.1056/NEJM200009283431307. - DOI - PubMed
Polman CH, Reingold SC, Banwell B, Clanet M, Cohen JA, Filippi M, Fujihara K, Havrdova E, Hutchinson M, Kappos L, Lublin FD, Montalban X, O'Connor P, Sandberg-Wollheim M, Thompson AJ, Waubant E, Weinshenker B, Wolinsky JS. Diagnostic criteria for multiple sclerosis: 2010 revisions to the McDonald criteria. Ann Neurol. 2011;69(2):292–302. doi: 10.1002/ana.22366. - DOI - PMC - PubMed
Putzki N, Pfriem A, Limmroth V, Yaldizli O, Tettenborn B, Diener HC, Katsarava Z. Prevalence of migraine, tension-type headache and trigeminal neuralgia in multiple sclerosis. Eur J Neurol. 2009;16(2):262–267. doi: 10.1111/j.1468-1331.2008.02406.x. - DOI - PubMed
Raskin NH, Hosobuchi Y, Lamb S. Headache may arise from perturbation of brain. Headache. 1987;27(8):416–420. doi: 10.1111/j.1526-4610.1987.hed2708416.x. - DOI - PubMed
Sandyk R, Awerbuch GI. The co-occurrence of multiple sclerosis and migraine headache: the serotoninergic link. Int J Neurosci. 1994;76(3–4):249–257. doi: 10.3109/00207459408986007. - DOI - PubMed
Swanton JK, Fernando K, Dalton CM, Miszkiel KA, Thompson AJ, Plant GT, Miller DH. Modification of MRI criteria for multiple sclerosis in patients with clinically isolated syndromes. J Neurol Neurosurg Psychiatry. 2006;77(7):830–833. doi: 10.1136/jnnp.2005.073247. - DOI - PMC - PubMed
Tortorella P, Rocca MA, Colombo B, Annovazzi P, Comi G, Filippi M. Assessment of MRI abnormalities of the brainstem from patients with migraine and multiple sclerosis. J Neurol Sci. 2006;244(1–2):137–141. doi: 10.1016/j.jns.2006.01.015. - DOI - PubMed
Villani V, Prosperini L, Ciuffoli A, Pizzolato R, Salvetti M, Pozzilli C, Sette G. Primary headache and multiple sclerosis: preliminary results of a prospective study. Neurol Sci. 2008;29(Suppl 1):S146–S148. doi: 10.1007/s10072-008-0908-3. - DOI - PubMed
Yetimalar Y, Secil Y, Inceoglu AK, Eren S, Basoglu M. Unusual primary manifestations of multiple sclerosis. N Z Med J. 2008;121(1277):47–59. - PubMed
Zorzon M, Zivadinov R, Nasuelli D, Dolfini P, Bosco A, Bratina A, Tommasi MA, Locatelli L, Cazzato G. Risk factors of multiple sclerosis: a case–control study. Neurol Sci. 2003;24(4):242–247. doi: 10.1007/s10072-003-0147-6. - DOI - PubMed